On April 21, Ashley Delaney brought his father-in-law to the Goa Medical College and Hospital, the largest public hospital in the small southwestern Indian state. The hospital was in chaos and the wards were packed, with all 708 covid beds occupied—so 69-year-old Joseph Paul Alvares, a cancer survivor, had to lie on a gurney for nearly three days for a bed to become available. The bathrooms were so filthy that many patients chose to wear adult diapers. And when one covid-positive man developed seizures, the hospital staff—seemingly unable to cope— tethered him to the bedposts with bandages. Delaney was so disturbed by what he saw that he decided to stay by his father-in-law’s side in case things took a turn for the worse. Soon enough, they did.
On the morning of April 28, several patients’ monitors started to flash and indicate that they were in distress, but the hospital staff didn’t respond. When Delaney went over to investigate, he saw that the patients—around 10 to 12 of them, as he later recalled—had died. He wasn’t a doctor, but it looked as if there had been a problem with the oxygen supplies. Delaney alerted several nurses and doctors, who told him that they had already complained to the administration but had been brushed aside. On May 2, the incident repeated itself. This time 12 patients died. On May 3, the number who died that night rose to 14. Delaney observed that in each case, a drop in oxygen had occurred between 2 a.m. and 6 a.m. It seemed to him that oxygen supplies were running out night after night, causing patients to asphyxiate.
On May 4, after Delaney had been observing the covid wards for nearly two weeks, an entire ward ran out of oxygen. He saw a chance to save everyone affected—all the patients were still alive, though struggling—but when he approached staff, they confided that they were afraid of reprisals from the hospital administration if they raised their voices. After two patients died, he went public with his findings.
Delaney, a 39-year-old IT consultant, already had a penchant for activism. At the start of the pandemic, he had delivered essential supplies to migrant workers. He enlisted his wife, a fashion designer, to make protective masks, which the couple distributed for free to frontline workers. Now he turned to the same place where other desperate, internet-savvy Indians were seeking help during the overwhelming second wave: social media.
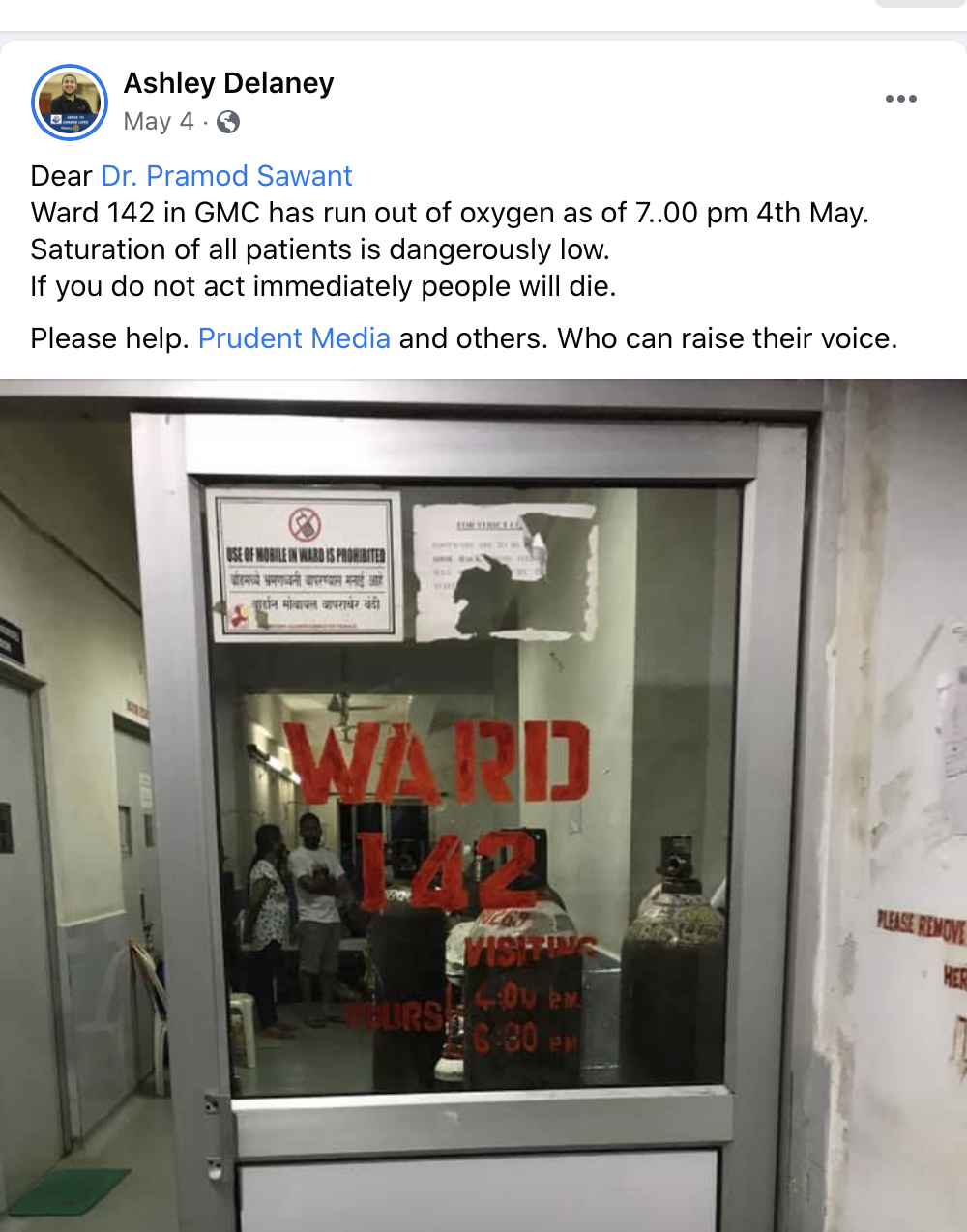
Delaney wrote a whistleblowing Facebook post that he shared with his 2,700 friends, tagging Goa’s chief minister, Pramod Sawant: “Ward 142 in GMC has run out of oxygen as of 7.00 pm 4th May. Saturation of all patients is dangerously low. If you do not act immediately people will die.” The post went viral. The very next day, Sawant appeared at the hospital to meet with staff and brief the press.
An internal investigation would later show that on the nights of May 2 and 3, 23 people had died because of a drop in oxygen levels, just as Delaney said. (The other deaths were attributed to covid-related causes.) Lawyers appearing on behalf of the state government at a later hearing claimed that the disruption in the supply had occurred because the tractor carrying the oxygen had difficulty “maneuvering” on hospital grounds. The tractor was linked to the loss of at least 83 lives in five nights.
America may seem to be approaching the end of the pandemic, but covid-19 remains a surging catastrophe in India, with more than 30 million people infected and more than 400,000 deaths—official figures that many believe are far below the real numbers. A more likely scenario, the New York Times reported on May 25, is that 539 million people have been infected and more than 1.6 million are dead. On June 27, the Wall Street Journal published figures from the University of Washington’s Institute for Health Metrics and Evaluation, whose modeling also suggests that India is undercounting. The institute estimates the death toll at over 1.1 million, or three times the official figure.
But the crisis was not an unavoidable tragedy. Even the new delta variant discovered to be sweeping through the country was not some terrible random error. Instead, the catastrophe that has struck millions of Indians is the direct outcome of the government’s failures: its failure to plan ahead by increasing hospital capacity and acquiring medicines; its failure to figure out contact tracing, collect adequate data, and purchase vaccines. Even after it became clear that a second wave was inevitable, the government went ahead with superspreader events that served its own political purposes—and gave the virus a new opportunity. And at the center of the crisis—paying little attention to science, seemingly refusing to heed good advice, and appearing concerned primarily with holding on to power at any cost—stands India’s Prime Minister Narendra Modi, a Hindu nationalist whose arrogance and underpreparedness have cost the country an incalculable amount.
One crisis caused another
In March 2020, the early days of the pandemic, Modi announced a surprise and strict 21-day national lockdown. At the time India had reported just 360 cases and seven deaths, according to the WHO. Modi’s decision was applauded as proactive, but it was also poorly managed: he gave India’s 1.39 billion people less than four hours to prepare before the lockdown went into effect, triggering the largest mass migration in the history of the subcontinent since the Partition of India in 1947. Millions of daily wage workers—estimates range from 10 million to 80 million—scrambled to return to their homes in the rural hinterland, but with public transport closed, many were forced to walk hundreds of kilometers. In its attempt to prevent one disaster, the government caused another. A humanitarian crisis now unfolded live on India’s TV screens as nearly 1,000 migrants died from various lockdown-related causes—traffic accidents, starvation, and even police brutality as officers mercilessly enforced the rules. Not only that, but the migration carried the virus, which had been concentrated in urban centers, into every corner of the country.
It wasn’t long before Indians could look to positive news, though. In April 2020, the Serum Institute of India—the world’s biggest vaccine manufacturer—announced that it would be producing millions of doses of the Oxford-AstraZeneca vaccine, including up to 60 million doses in 2020 and 400 million in 2021. Serum produces more than 1.5 billion doses of vaccines every year, so it wasn’t a stretch to imagine that it was up to the task. The company’s billionaire chief executive, Adar Poonawalla, told Reuters that Modi was “very closely” involved with the company’s plans.
But while the prime minister was later photographed visiting the Serum Institute, the Indian government didn’t actually enter into an agreement with the manufacturer—nor did it help it to ramp up production. In the US, the government had launched Operation Warp Speed to accelerate the federal response to the pandemic; in Britain, Downing Street had funded the development of the AstraZeneca vaccine with an £84 million ($117 million) grant and an order for up to 340 million doses. Modi, on the other hand, didn’t secure vaccines from the manufacturer in his own backyard.
India’s loss was the world’s gain: Serum signed contracts with COVAX, a vaccine-sharing partnership, and other countries including Canada and the United Kingdom. It wasn’t until January 2021 that the Indian government placed its first order—by which time virtually all of Serum’s stock was spoken for. New Delhi later dealt with the problem by forcing a freeze on exports until the end of 2021, dealing a severe blow to 92 of the world’s poorest countries, which were relying on Serum for their supply of the AstraZeneca vaccine.
On May 31, 2020, Indians emerged out of the strict lockdown to a situation more precarious than before. More than 140 million people had lost their jobs, and the unemployment rate had rocketed from 8% to 26%. The government hadn’t used the extra time to build new hospitals, better equip more than a handful of old ones, or stockpile medication. The lockdown had taken the virus to India’s villages, where medical oxygen was a scarce commodity in the best of circumstances.
“The idea behind the lockdown was to prepare,” says Ramanan Laxminarayan, the founder and director of the Center for Disease Dynamics, Economics & Policy, a public health organization in Washington, DC. “That didn’t seem to have happened.”
Instead, India exported vital supplies: twice as much oxygen as the year before, and close to 1.1 million units of the antiviral drug remdesivir, were sold to other countries. As some people, including President Trump, touted hydroxychloroquine as a remedy, India sent the United States 50 million tablets. And as soon as Serum was producing vaccines, India exported those as well. Before the anniversary of the pandemic, the government gave away more than 66 million doses to 95 countries in a diplomatic effort it called Vaccine Maitri, or Vaccine Friendship.
“Goa was left to the dogs”
By September 2020, India had the world’s fastest-growing outbreak of covid-19 in absolute numbers, according to the WHO, with between 5 and 6 million infections. In a nationally televised address on October 20, Modi urged people not to let their guard down and told them to wear masks—then immediately undercut his message. “Out of every million, we have around 83 deaths,” he told a TV audience. The numbers drew scrutiny, with concerns that there was substantial undercounting—no surprise given that the previous year he’d been accused of suppressing his own government’s report on the unemployment rate because it showed a 45-year high.
Then, in November, a doctor named Arun Njanappilly Madhavan published a spreadsheet that showed a discrepancy between official death figures and the numbers that he and a group of volunteers had collected. They’d scoured newspaper obituary notices and TV reports in Kerala during India’s first wave. “In Kerala itself around 60 to 70% of deaths were not counted,” says Arun. “People who had underlying conditions or those who had tested negative just before dying were not counted as covid-positive deaths.”
Kerala’s handling of the pandemic is widely considered one of the few bright spots in an otherwise dismal landscape. If the undercounting there was so bad, suggested Arun, it was likely far worse elsewhere.
But voices like his were drowned out by the federal government’s messaging, which suggested that India had somehow outwitted the virus. The hype was so strong that even some medical professionals bought into it. A Harvard Medical School professor told the financial daily Mint that “the pandemic has behaved in a very unique way in India.”
“The real harm in undercounting is that people will take the pandemic lightly,” says Arun. “If supposedly few people are dying due to covid, the public will think it doesn’t kill, and they won’t change their behavior.” In fact, by mid-December India had reached yet another somber milestone: it recorded its 10 millionth infection. It was only the second country to do so, after the US.
The government hadn’t used the first lockdown wisely, but December was its chance to set things right, says Gagandeep Kang, a professor of microbiology at the Christian Medical College in Vellore, Tamil Nadu. She says that a number of tactics—ramping up sequencing, studying public behavior, collecting more data, refusing permission for superspreader events, and starting the vaccine rollout earlier than planned—would have saved many lives during the now-inevitable second wave.
Instead, she says, the government continued its “top-down approach,” in which bureaucrats rather than scientists and health-care professionals were making decisions.
“We live in a very unequal society,” she says. “So we need to engage people and build partnerships at a granular level if we are to effectively deliver information and resources.”
In December the government of Goa let its guard down entirely. The state is heavily reliant on tourism, which makes up nearly 17% of its income. The bulk of the tourists show up in December to celebrate Christmas and New Year on sandy beaches with raves and fireworks.
Vivek Menezes, a Goan journalist, says that the state’s reputation as “the place to be” had not faded during the pandemic. “It’s the place for India’s wealthy and for Bollywood, and therefore it’s the place for India,” Menezes says. The pandemic had kept foreign tourists from visiting, but domestic holidaymakers poured in. Some states, such as Maharashtra, had placed restrictions at their borders; others, like Kerala, had a strict policy of contact tracing. In Goa, visitors didn’t even have to show a negative covid test. And the state’s masking policy extended only to health-care workers, visitors to health-care facilities, and people showing symptoms. “Goa was left to the dogs,” says Menezes.
The world’s largest superspreader
India started 2021 having registered nearly 150,000 deaths. Only then, in January, did the government place its first vaccine order, and it was for a shockingly low amount—just 11 million doses of Covishield, the Indian version of the AstraZeneca vaccine. It also ordered 5.5 million doses of Covaxin, a locally developed vaccine that has yet to publish efficacy data. Those orders fell far short of what the country actually needed. Subhash Salunke, a senior advisor to the independent Public Health Foundation of India, estimates that 1.4 billion doses would have been required to fully vaccinate all eligible adults.
On January 28, in an address to the World Economic Forum in Davos, Modi declared that India had “saved humanity from a big disaster by containing corona effectively.” His government then gave the go-ahead for the Kumbh Mela, a Hindu festival that attracts crushing throngs of millions of people to the holy city of Haridwar in the northern state of Uttarakhand, which is famous for its temples and pilgrimage sites. When the state’s former chief minister suggested that the festival should be “symbolic” this year given the circumstances, he was fired.
A senior politician in the prime minister’s Bharatiya Janata Party told the Indian magazine The Caravan that the federal government had its eye on the forthcoming state elections and didn’t want to lose the support of religious leaders. As it turned out, the Kumbh wasn’t just any superspreader event—with a reported 9.1 million people in attendance, it was the world’s largest superspreader event. “Any person with a basic textbook on public health would have told you this was not the time,” says Kang.
The Indian government only placed its first vaccine order in January 2021, after having registered nearly 150,000 deaths. Even then, it was for a shockingly low amount—11 million doses of Covishield and 5.5 million doses of Covaxin for a country of 1.3 billion.
In February Salunke, the public health expert, was working in an agrarian district in the western state of Maharashtra when he noticed that the virus was transmitting “much faster” than before. It was affecting entire families.
“I felt we were dealing with an agent that had changed or appeared to have changed,” he says. “I started to investigate.” Salunke, it now turns out, had found one mutation of a variant that had been detected in India the previous October. He suspected that the variant, now known as delta, was about to run rampant. It did. It is now in more than 90 countries.
“I went to all those who are responsible and those who matter—whether district level officials or bureaucrats at the central level, you name it. Everyone who I knew I immediately shared this information with,” he says.
Salunke’s discovery doesn’t appear to have affected the official response. Even as the second wave was accelerating and after the WHO designated the new mutation “a variant of interest” on April 4, Modi kept up his hectic schedule ahead of state elections in West Bengal, personally appearing at numerous public rallies.
At one point he gloated about the size of the crowd he had attracted: “In all directions I see huge crowds of people … I have never seen such crowds at a rally.”
“The rallies were a direct message from the leadership that the virus was gone,” says Laxminarayan of the Center for Disease Dynamics, Economics & Policy.
The second wave filled hospitals, which quickly ran out of beds, oxygen, and medication, forcing gasping patients to wait—and then die—in homes, in parking lots, and on sidewalks. Crematoriums had to build makeshift pyres to keep up with the demand, and there were reports that the outpouring of ash drifted so far it stained clothes a kilometer away. Many poor people couldn’t even afford to pay for funeral rites and immersed the bodies of their loved ones directly into the River Ganges, which led hundreds of corpses to wash up on the banks in several states. Alongside these apocalyptic scenes came the news that deadly fungal infections were overwhelming covid patients, likely as a result of lower infection control and overreliance on steroids in treating the virus.
Chaos continues; Delta spreads
And all along, there has been Modi. The prime minister had been the face of India’s fight against the pandemic—literally: his headshot appears prominently on the certificate given to people who get their vaccine. But after the second wave, his premature triumphalism was mocked and his lack of preparedness derided widely. Since then, he has gone largely missing from the public eye, leaving it to colleagues to place the blame elsewhere, most notably—and inaccurately—on the government’s political opposition. As a result, Indians have been left to face the biggest national crisis of their lifetime on their own.
This abandonment has created a sense of camaraderie among some groups of Indians, with many using social media and WhatsApp to help each other out by sharing information about hospital beds and oxygen cylinders. They have also organized on the ground, distributing meals to those in need.
“The [BJP] rallies were a direct message from the leadership that the virus was gone.”
Ramanan Laxminarayan, the Center for Disease Dynamics, Economics & Policy
But the leadership vacuum has also produced a huge market for profiteers and scammers at the highest levels. In May, opposition politicians accused a leader of the ruling BJP party, Tejaswi Surya, of taking part in a vaccine commission scam. And the health minister of Goa, Vishwajit Rane, was forced to deny claims that he played a part in a scam involving the purchase of ventilators. Even the prime minister’s signature covid relief fund, PM Cares, came under fire after it spent Rs 2,250 crore (over $300 million) on 60,000 ventilators that doctors later complained were faulty and “too risky to use.” The fund, which attracted at least $423 million in donations, has also raised concerns about corruption and lack of transparency.
A successful vaccination agenda might have helped erase the memory of the string of missteps, but under Modi it has only been one technocratic mistake after another. At the end of May, with far fewer vaccines in hand than it needs, the government announced plans to start mixing doses of different vaccine types. And at the height of the second wave, it introduced Co-WIN, an online booking system that was mandatory for anyone under 45 who was trying to get vaccinated. The system, which had been under scrutiny for months, was disastrous: not only did it automatically exclude those who do not use computers and smartphones, but it was also hit by bugs and overwhelmed by people desperate to get protection.
And then there’s cost. While the government covered the cost of vaccination for health-care staff, frontline workers, and those over 45, it expected people between the ages of 18 and 44 to pay for their own shots. India was the only major country to pass on this cost to the public. Most paid around Rs 900 ($12) for one shot, but some reported being charged as much as Rs 1800 ($25), an astronomical sum in a country where 134 million people live on less than $2 a day. In yet another unprecedented move, the government told individual states that it was up to them to purchase vaccines for the under-45s. “This was another googly,” says Laxminarayan, who called the government’s decision “bizarre.” India was one of only two countries in the world to adopt this model—the other being Brazil, which has also registered hundreds of thousands of deaths.
The vaccination plans were so unrealistic and unfair that the Supreme Court weighed in on May 31, telling the government to “see what’s happening across the country.”
The court described some of the government’s actions as “arbitrary and irrational” and demanded a “fresh review of its vaccination policy.” In early June, the government responded to the rebuke by agreeing to procure vaccines for everyone who is eligible and supply them to the states for free. However, in order to get a slot, many Indians still have to access Co-WIN, the error-prone online service. It’s the sort of chaos that they do not need more of—but continue to face.
What the next wave looks like
In early May, Ashley Delaney, the Goa Medical College whistleblower who witnessed the overnight oxygen failures, came across yet another patient who needed his help. Sumita Datta, an assistant professor of economics, had been admitted to the hospital with covid but was left unattended for around 14 hours.
“I was drifting in and out of sleep, but none of the staff bothered with me,” she says. Delaney noticed Datta and gave her something to eat and drink. He also took her for her tests, even as his father-in-law’s condition deteriorated.
On May 23, Delaney’s father-in-law died of covid-19. Datta, who is 38, survived, although she was diagnosed with covid-related pneumonia. A CT scan showed that more than 50% of her lung tissue was infected. Six days later she was discharged, but she was bedridden for two more weeks with chest pains, a rapid pulse, and general exhaustion.
Today, India’s second wave has largely subsided. But the threat is far from over. A version of the delta variant known as delta plus, first reported on June 11 and said to be even more transmissible, has already been detected in 12 states. And as of June 27 only 4% of Indians were fully vaccinated, according to a Bloomberg study.
Now India’s health-care experts have started warning of a third wave that could come as early as September. Salunke is among those who believe that it will hit those under 18 and that health-care workers must be given the specialized training required to care for pediatric patients on ventilators. To save lives, the Indian government has to do more of everything, he says, including getting more people vaccinated and procuring more drugs for the rapidly increasing number of fungal infections.
“We have to have a plan for until the end of December 2021, and then we have to prepare for up to 2022,” he says. “This won’t go away for at least the next two years.”
Meanwhile, in Goa, Datta is still shaken. When she returned to work after weeks in bed, she found herself unable to focus for more than 20 minutes at a time. Three days later she was home in bed once more. She says she is “terrified” about the future of the pandemic in India and feels caught at the center of a web of mistakes and missteps. Feeling helpless, she wonders: “What do we do?”
This story is part of the Pandemic Technology Project, supported by the Rockefeller Foundation.


{kind=link}
Recent Comments